Why Provider Data Keeps Breaking — And Why Patching the Symptoms Doesn't Work
Provider directories don't fail because of bad luck or sloppy work. They fail because they're built on fragmented sources, self-reported data, infrequent refresh cycles, and no validation layer. Here's what it actually takes to fix the architecture, not just the symptoms.

For decades, the healthcare industry has treated provider data like a leaky pipe. We wrap it in tape, place a bucket underneath, and hope it holds until the next quarter. But the pipe keeps bursting.
Provider directories have failed for years because they rely on a fundamentally broken foundation. We are not dealing with a simple maintenance issue. We are dealing with an architectural failure built on fragmented, self-reported data from misaligned sources. Health plans, providers, and government registries all maintain separate records. They do not talk to each other, and worse, no single system of truth exists between them.
At Candor Health, we look past the symptoms. We focus on why this problem persists year after year. Through our work with payers and health systems, I have seen firsthand that provider data consistently breaks down due to four root causes.
1. Fragmented sources
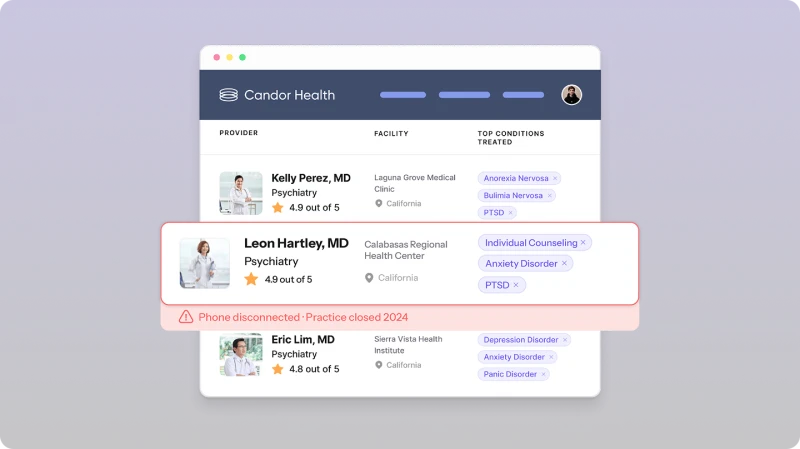
Healthcare organizations operate in silos. A health plan might use one system for credentialing and another for claims. The local health system has its own internal roster, while government registries maintain completely separate databases. When these systems refuse to communicate, data fractures. You end up with five different addresses for a single physician, and no easy way to determine which one is right.
2. Self-reported data
The industry relies heavily on providers or office managers to manually update their information. This creates a massive administrative burden. When updating a directory requires filling out forms across dozens of different health plans, the task inevitably falls to the bottom of the pile. Relying on self-reported data means relying on human memory and available time, both of which are in short supply in clinical settings.
3. Infrequent refresh cycles
Healthcare moves fast. Providers change practices, retire, or adjust their panel status daily. Yet, the systems designed to track them often operate on quarterly or even annual refresh cycles. By the time a directory update goes live, the information is already obsolete. You cannot manage a dynamic network with static snapshots.
4. No validation layer
Perhaps the biggest missing piece is validation. Data enters the system, and organizations accept it at face value. Without a rigorous, automated validation layer to verify that a provider actually practices at a specific location on the days claimed, bad data simply overwrites good data.
Moving beyond the symptoms
Patching the symptoms by throwing more administrative staff at the problem or running annual clean-up campaigns will never fix provider directories. To achieve true network adequacy and operational efficiency, we have to address these four root causes head-on.
At Candor Health, we built our platform to do exactly that. We do not just aggregate data; we validate, continuously refresh, and create a single, reliable source of truth that health systems and payers can trust.
We want to show you exactly what the current landscape looks like. Soon, we will publish a comprehensive Provider Accuracy Study that examines the real state of provider network data and the exact cost of these failing systems.
Standardize provider roster ingestion, reduce reconciliation overhead, and improve provider directory reliability with Candor Health.

Sury Agarwal is on a mission to transform how healthcare organizations access, manage, and trust provider data. Candor’s AI-powered platform supports payers, digital health companies, and provider groups with care navigation, referral management, network strategy, and regulatory compliance. Sury brings 12+ years of experience tackling complex data challenges. Previously, he was VP of Engineering and part of the founding team at Moat, which was acquired by Oracle for $850M in 2017. He is a Cornell University graduate.
More Posts
CMS Is Publishing Your Provider Directory: Publicly, Daily, and by Name

The Overlooked Bottleneck of Provider Data Accuracy

Provider Data Accuracy Without Compromising Network Adequacy