Finding the Right Doctor Is a Data Problem in Disguise
For the first episode of Candid Conversations, Candor Health CEO Sury Agarwal sat down with Sameer Sethi, former Chief AI and Data Officer at Hackensack Meridian Health to find out where it all went wrong.

Host

Sury Agarwal
Guests

Sameer Sethi
In theory, finding the right doctor should be a straightforward task. Yet, most patients still can't answer a deceptively simple question: how do I find the best provider for my specific care needs?
The problem isn’t just inside the search experience, it’s underneath it. Provider data, the information describing what a clinician specializes in, what conditions they treat, what procedures they perform, is among the most nuanced, inconsistently maintained, and poorly structured data in all of healthcare. Better search built on top of incomplete data doesn't solve the problem. It just returns the wrong answer faster.
For the first episode of Candid Conversations, Candor Health CEO Sury Agarwal sat down with Sameer Sethi, former Chief AI and Data Officer at Hackensack Meridian Health, who has spent his career at the intersection of data quality and clinical operations across some of the largest health systems in the country, focused on the tools and systems responsible for digitizing and interconnecting our healthcare system. Now, after more than two decades in the industry, he helps us understand where it all went wrong.
Before the Search Bar
Why is finding a doctor so difficult? Sethi offers a two-part diagnosis. Healthcare, he explained, lacks a strong user experience, an interface that patients can remember, appreciate, and meaningfully engage with. Unlike retail giants like Amazon, healthcare organizations have never excelled at building sticky, consumer-grade touchpoints that resonate with users.
But the real challenge starts far below the surface. “It’s all about the data,” Sethi explains. Advanced tools like artificial intelligence (AI) have incredible potential to transform healthcare, but they’re only as strong as the information they’re given.
"AI is not magic. It uses an underlying dataset. And if the data isn’t there, AI can’t deliver."
Specialty Is Not Enough
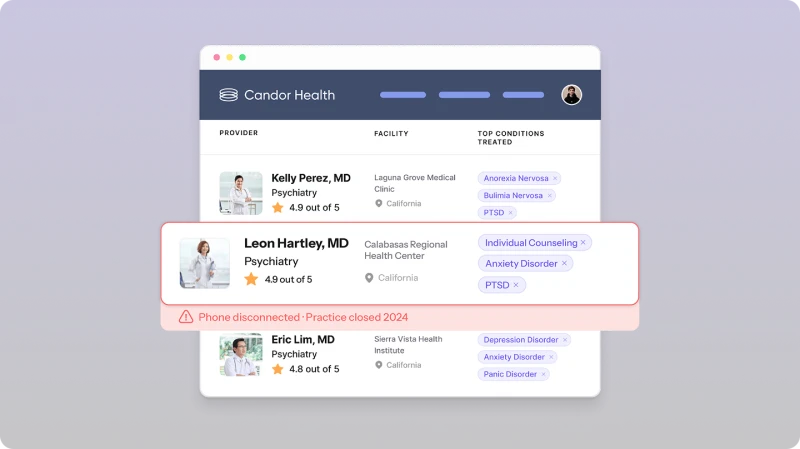
Taxonomy is an important piece of the puzzle. When patients or referring physicians look for a specialist, the available filters are mostly specialty-based: orthopedics, cardiology, neurology, and so on. But specialty designations are broad categories, and even those categories, Sethi noted, aren't always structured in ways that are useful at the moment of care.
"The finding-a-doctor feature has always just focused on specialties. And the sad part is we as health systems don't do even a good job categorizing that in a way that would be most valuable at the time of selection."
What's needed, he argued, is a multi-factor logic built around what matters to a patient at the point of decision: the specific procedure or condition in question, how frequently a clinician performs that procedure, available quality measures, scheduling availability, and proximity. Each of those inputs exists somewhere in a health system's data, yet none of them are aggregated and surfaced in a way that provides an actionable answer to the end user.
Sethi pointed to the logic behind modern consumer search. When users shop online, results aren't filtered by product category alone. They're surfaced through a complex algorithm that accounts for numerous factors such as relevance, volume, ratings, availability, and a user's search history. Healthcare has all the underlying ingredients, Sethi explained. It just hasn't built the logic to put them together.
Physicians Are Working From the Same Broken Map
Zooming out, Agarwal raised another key dimension of the problem: physicians making referrals are navigating the same fragmented information landscape as their patients.
Previously, Sethi had built tools to address this directly. When his team began developing physician-facing referral search capabilities, they discovered that clinicians didn't have reliable access to granular procedure-level data about their colleagues either. For instance, a referring physician might know that a colleague is an orthopedic surgeon, but they wouldn't know that surgeon's experience with specific procedures unless they had a personal relationship or had looked it up through a system that rarely surfaced that level of detail.
"What the physician is expecting is something a bit more medically focused. If they type 'buckle fracture,' that should connect to a procedure code, and the system should surface clinicians who actually perform that procedure."
The fix he described is far from impossible. The data exists in claims records and clinical systems. What it does require, however, is someone capable of extracting it, transforming it into something usable, and wiring it to the EHR workflow so the physician can make a reliable referral decision in real time. The capability is there but the focus and investment to build it is not.
The AI Shortcut and Its Risks
According to a recent study, a quarter of patients now use AI tools to influence their choice of provider, treating ChatGPT and similar general-purpose tools on par with a primary care physician's recommendation. For Agarwal, that raises a question of accountability: when a patient ends up with the wrong specialist because they navigated there using a general AI, who owns that?
Sethi's answer was careful. Health systems shouldn't be held responsible for outputs generated by tools they didn't build and didn't ask their patients to use. But that's not the end of the responsibility conversation. The reason patients are turning to general AI is because nothing better has been made available to them.
"Health systems need to provide that kind of chat interface to patients, so they can search for providers using reliable information. The tool should be built and grounded on the right data. That's where responsibility lives."
The deeper issue, he argued, is that general-purpose AI is being treated as a universal tool for everything, including tasks it isn't designed or grounded to handle. In healthcare specifically, that mismatch carries real risk. These tools are built to answer confidently. They aren't built to say "I don't know," Sethi explained. Applied to provider selection or clinical triage, that confidence gap can lead patients toward the wrong care.
His position wasn't anti-AI. It was pro-specialization: A crane is built for construction, a car is built for transportation, and using one in place of the other isn't an innovation; it's user error.
"People should not be using ChatGPT to find a doctor. If you go to the right AI tool and ask the right question, you should get the right answer."
The Investment Gap
A running thread through the conversation was the gap between what patients now expect and what health systems have historically been willing or able to invest in.
Post-COVID, Sethi argued, the baseline changed. Patients who once resisted telehealth are now requesting it; with this shift comes increased demand for seamless, high-touch interactions. As a generation of digital-first consumers enters the marketplace, organizations have a lot to learn from companies like Amazon.
"A health system is able to engage with the patient maybe once or twice a year. Amazon engages with you eleven times a year. There's something to be learned from that."
So far, digital investments haven’t caught up to consumer expectations. Health systems are building for compliance and operational necessity. The deliberate, consumer-grade investment in data infrastructure and digital experience that retailers make as a matter of competitive survival hasn't made its way into healthcare. At least, not at scale.
Sethi pointed out that none of this is a technology gap. Health systems have the tools. They have the data too, even if it's messy and scattered. What they haven't done is decide that data readiness and digital experience deserve the same strategic attention as any other business priority, rather than being filed away as IT upkeep.
Sethi’s Blueprint
When asked for a concrete picture of what a solved state would require, Sethi described three layers that have to be present and connected.
First is clean, structured, purpose-built data. Someone has to take the clinical and claims data that already exists, extract the relevant attributes, transform them into usable form, and make them available. Name, location, schedule, procedure volume, quality scores: these need to be structured for the specific purpose of matching patients and physicians, not just for billing or compliance.
Next comes a consumer-grade digital experience. The interface needs the same intentionality retailers bring to product search. It has to be treated as a real investment in patient engagement.
The third piece is the logic layer in between. Someone has to build the matching intelligence that can translate a user’s query into the codes and attributes that live in the data, and return a result that's clinically relevant.
"First we focus on the underlying data, then comes the digital experience. Once those two sides are complete, the right logic has to bring it all together."
Candid Conversations is a series by Candor Health featuring honest discussions with the experts closest to healthcare’s most persistent data challenges.
Standardize provider roster ingestion, reduce reconciliation overhead, and improve provider directory reliability with Candor Health.
More Posts
CMS Is Publishing Your Provider Directory: Publicly, Daily, and by Name

The Overlooked Bottleneck of Provider Data Accuracy

Provider Data Accuracy Without Compromising Network Adequacy